RU58841 — topical science at the follicle.
RU58841 (PSK-3841) is a non-steroidal anti-androgen explored for androgenetic alopecia. This site explains how it targets scalp receptors, why it is not licensed in the UK, and what that means if you are weighing options with your clinician.
We separate mechanism from marketing noise, compare RU58841 with finasteride, and place pyrilutamide in context. Nothing here replaces medical advice.
- Local
- Receptor focus
- NSAA
- Class
- Trial
- Stage halted

Experimental
Not an MHRA product.
Androgenetic hair thinning affects many adults in the UK. Clinicians commonly discuss minoxidil, finasteride, and occasionally dutasteride off-label, alongside lifestyle and surgical routes. RU58841 sits outside that licensed toolbox: it appeared in company-led research decades ago, showed promise in animal models and human scalp tissue experiments, yet never completed the regulatory path you would expect for a pharmacy medicine.
Readers arrive here with sensible questions. Does a topical anti-androgen spare systemic hormone shifts? Can you infer long-term safety from forum posts? How should you interpret before-and-after galleries that lack standardised photography? We answer in plain English, cite the limits of the literature, and point to our deep dives on side effects, practical application concerns, and community reports.
Topics
Pick a chapter.
Each page stands alone but links to neighbours so you can move from mechanism to risk without losing context.

Side effects
Irritation, systemic anecdotes, and data gaps.
Open →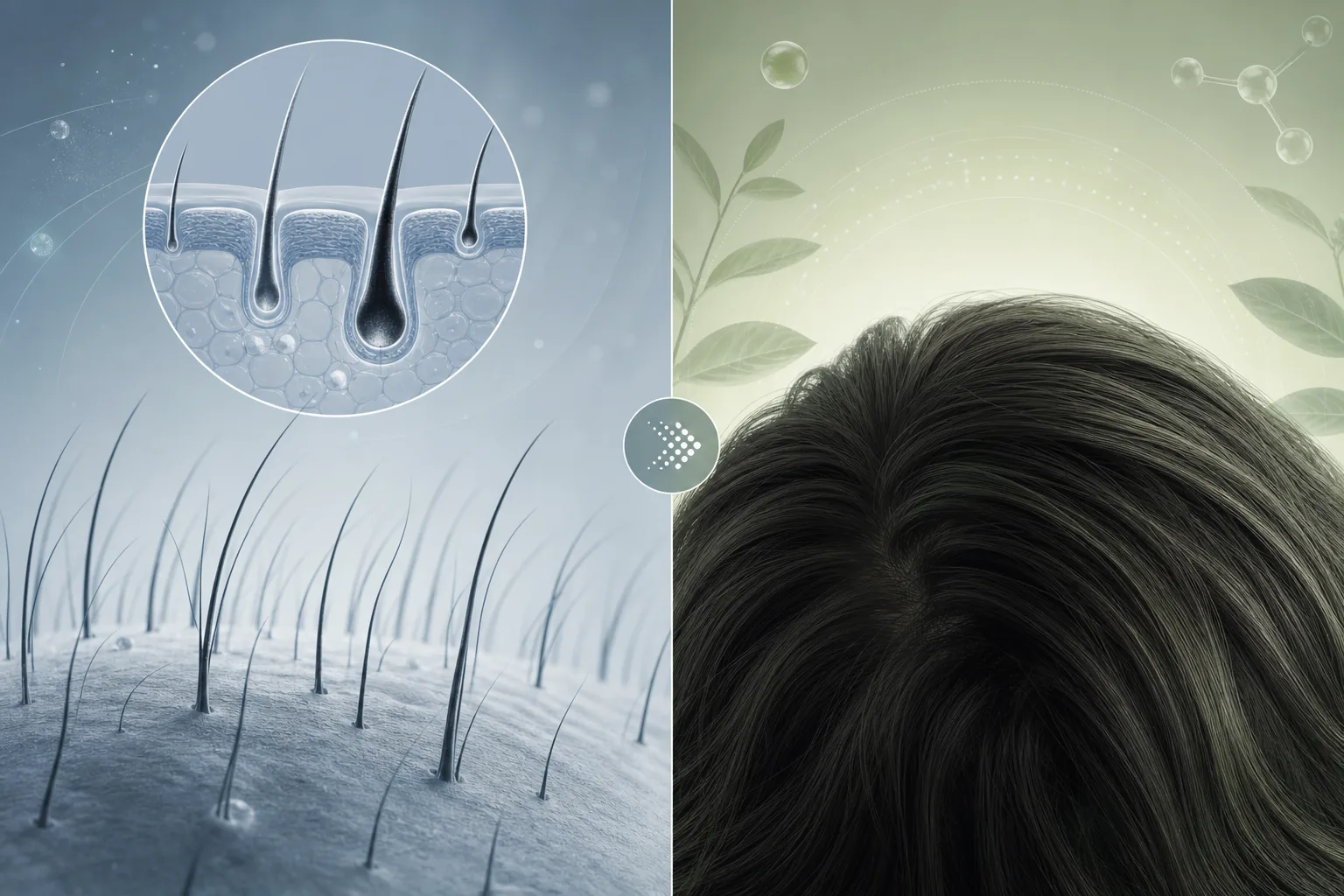
Before & after
Photos, timelines, and healthy scepticism.
Open →
vs Finasteride
Systemic DHT change versus local blockade.
Open →
vs Pyrilutamide
Another topical AR pathway under study.
Open →
How to use
Vehicles, contact rules, hygiene — general principles.
Open →
Is it safe?
Regulatory reality and informed caution.
Open →
About
Who writes this site and how we work.
Open →
Results & reviews
Patterns in self-reported journeys.
Open →Deep read
What believers and sceptics share.
Whether you first heard of RU58841 on a patient forum or in a chemistry blog, the same fact repeats: high-quality human trials are thin on the ground. Early work in the nineteen-eighties and nineties framed it as a selective antagonist at the androgen receptor. Animal data — including macaque models — hinted at cosmetically meaningful regrowth when delivery reached the follicle reliably. Human scalp studies existed in research settings, yet the compound stalled before the finish line of a marketed drug.
That pause matters. Licensing agencies want repeatable dosing, documented adverse events, manufacturing consistency, and long-term follow-up. When those pieces are missing, clinicians in the UK default to interventions with clearer dossiers. Our About page explains editorial independence; the short version is that we are not affiliated with supplement shops, compounding pharmacies, or grey-market vendors.
Mechanism in patient language
Dihydrotestosterone (DHT) tightens the miniaturisation screw on genetically susceptible follicles. Oral finasteride trims DHT production system-wide. RU58841, in contrast, is designed to sit on the receptor’s docking site in scalp tissue so DHT cannot trigger the same signalling cascade — at least where penetration and concentration are adequate. The distinction is not academic: it shapes which side-effect conversations belong on the table.
Penetration is the quiet variable. Skin barrier health, vehicle choice, application time, and overlap with minoxidil can all shift outcomes. Our How to use article sticks to hygiene and realism rather than recipe-sharing, because unsupervised compounding introduces its own risks — sterility, stability, and uncertain potency after shipping heat spikes.
Why comparisons go mainstream
People compare RU58841 to finasteride because both touch the androgen pathway, but the pharmacology diverges after that headline. They compare it to pyrilutamide (KX-826) because both belong to the newer wave of topical anti-androgens discussed online while formal access remains limited or trial-bound. Our twin pages walk through efficacy claims, safety narratives, and what is genuinely unknown.
For aesthetics, Before and after content needs a disciplined eye. Lighting shifts, wet versus dry hair, different angles, and concurrent treatments can exaggerate apparent change. We encourage documenting your own baseline with consistent rules if a specialist approves any plan — and we caution against chasing screenshots as proof of safety.
Ethics of sourcing chatter
We reference community patterns on Results and reviews with clear labelling: anecdotes are hypotheses, not endpoints. When someone describes palpitations, we note that causality is unproven without structured monitoring — mirrored on Side effects. Transparent uncertainty is more respectful than false precision.
If you live in the UK and want regulated care, start with a GP referral to dermatology or a trichology-versed clinician. Bring a list of every topical you use, including cosmeceuticals. Ask how they interpret blood tests, scalp examination, and whether photography belongs in your follow-up. Those steps remain the gold standard even as scientific Twitter argues molecule by molecule.
Additional context from dermatology reviews: the British Association of Dermatologists publishes patient-facing resources on common prescriptions; they help you compare what is standard of care with what remains investigational. The NHS hair loss overview likewise anchors expectations for first-line therapies available through UK services.
Formulation chemistry also deserves airtime. Many hobbyist vials mix powder into ethanol–propylene glycol vehicles without knowing oxidative degradation curves. A solution that darkens, precipitates, or smells sharply different week to week is not trivially “still fine.” Without chromatography, users guess potency. That reality pushes us back to the same advice: if an intervention matters to your health, involve someone who can measure and respond to adverse signals.
Psychology intersects pharmacology here. Hair loss isolates people; desperation is an understandable emotion, not a moral fault. Ethical writers should resist exploiting vulnerability with miracle language. Measured claims feel slower, yet they age better — and they align with how serious researchers discuss unfinished molecules.
Timeline honesty matters too. Hair cycling runs in months, not weekends. Any story that promises density jumps without acknowledging the telogen–anagen window deserves scepticism. When you read community write-ups, look for dates, concurrent changes to diet or stress, and whether photography stayed fixed on the same lens distance.
Summarising responsibly: RU58841 is a fascinating chapter in hair science, not a plug-and-play substitute for professional judgement. Use this hub to orient yourself, then let measurable clinical guidance lead the final call.
FAQ
Quick answers.
Mismatch between curiosity and regulation is normal. If you need tailored advice, consult a UK prescriber.
-
What is RU58841?
A non-steroidal anti-androgen investigated for topical hair loss. It competes with DHT at the receptor rather than suppressing DHT synthesis like oral finasteride.
-
Is it legal to buy in the UK?
Rules evolve and depend on product claims, import channels, and whether a substance is controlled. This site does not provide sourcing guidance. A solicitor or regulator is the right channel for specific cases.
-
Can women use topical anti-androgens?
Some androgen pathways matter in female pattern hair loss, but pregnancy risk categories and endocrine balance differ. Only a qualified clinician should recommend use, if at all.
-
Does topical mean zero systemic exposure?
No. Percutaneous absorption still occurs, especially with occlusive vehicles, broken skin, or frequent large-area application. “Local” is a goal, not a guarantee.
Stay curious, stay clinical.
Start with safety context, then compare mechanisms on our finasteride and pyrilutamide pages.
Open comparison